
My mother's occupational therapist handed me a gait belt during the second home visit after my mother's hip repair. She did not suggest it, she told me to use it every single time. I had used one at the rehab facility but I had never thought to buy one for the house. That afternoon I ordered the LiftAid belt from Amazon, and by the following morning I was using it. Within a week I stopped dreading the transfers. I stopped waking up with a tight lower back. And my mother, who is 87 and weighs about 142 pounds, actually said she felt more secure when I had hold of the belt than she ever had when I was grabbing her arms.
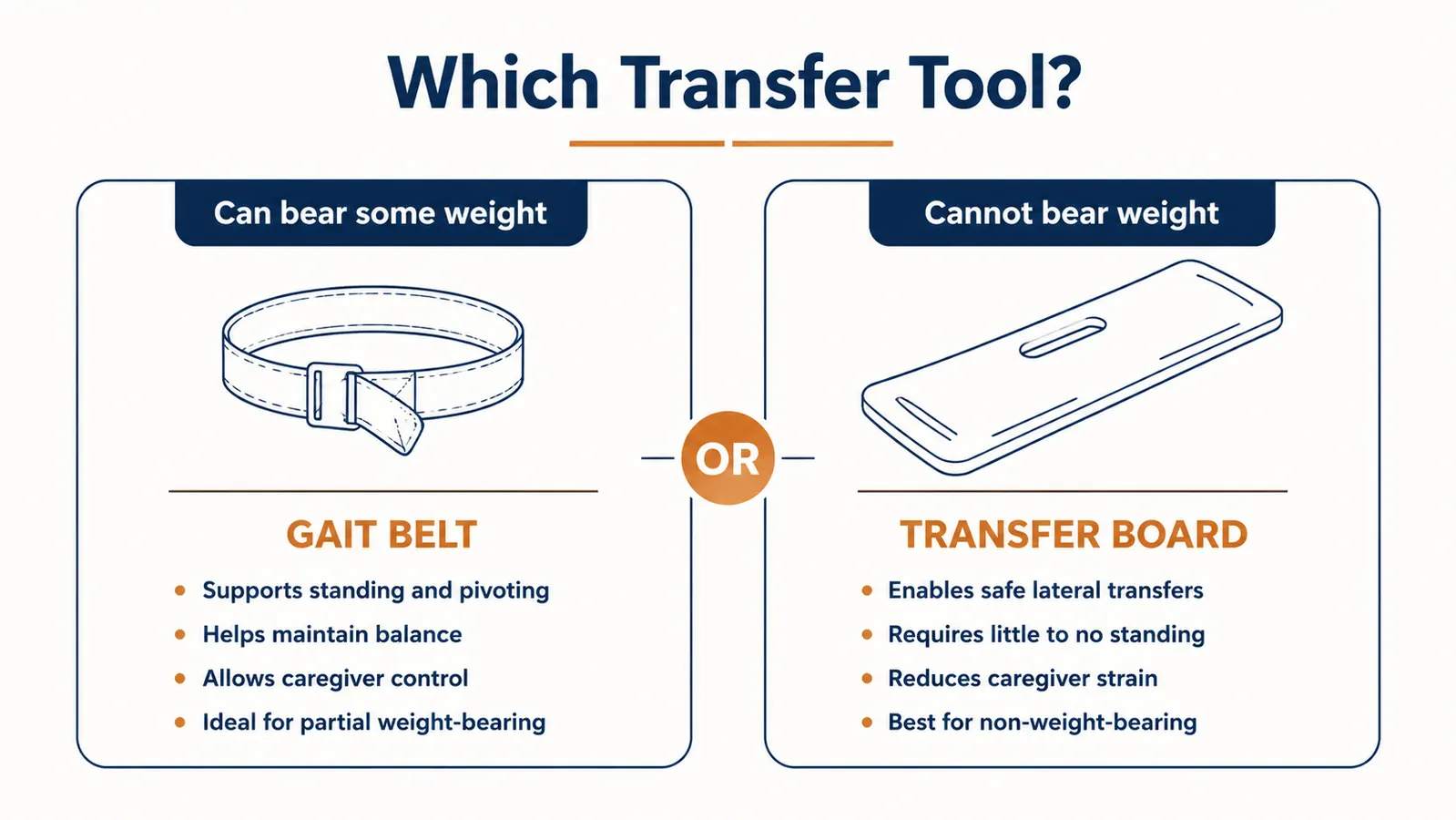
The question I get from other caregivers -- siblings, spouses, adult children who are newly in this role -- is always some version of the same thing: should I be using a gait belt, or should I get one of those sliding transfer boards? It is a fair question. Both tools exist to make patient transfers safer. But they solve different problems, and using the wrong one can actually make things harder or riskier. Here is how I think about the difference.
| attribute | left | right |
| attribute | left | right |
| attribute | left | right |
| attribute | left | right |
| attribute | left | right |
| attribute | left | right |
| attribute | left | right |
| attribute | left | right |
Where the Gait Belt Wins
The gait belt wins in the most common home caregiving scenario: your parent or spouse can still stand up if they have something to push against and someone steadying them. This is the weight-bearing patient. They are not lifting themselves from the floor unassisted, but when they get to the edge of the chair and push down with both hands and push up with both legs, they can get vertical. That leg drive is valuable. Your job as a caregiver is to harness it, not replace it.
When you wrap a gait belt around the patient's waist and buckle it snug, you now have a real handle at their center of gravity. Not their arm, which can be injured. Not their waistband, which can slip or hurt them. The belt. When they push up, you lift and guide from the belt, and the two of you are working together. The physics of this are genuinely different from trying to support someone by the arm. Your lower back stays more neutral because you are not reaching across or up, you are pulling from a low, stable point. The LiftAid belt has loops along the back panel that give you multiple grip options, which matters when you are tall and your patient is short or when the chair height puts you at an awkward angle.
The other thing the gait belt wins on is portability and simplicity. You put it on the patient before the transfer, and you take it off after. No positioning boards, no slide sheets, no furniture arrangement required. It takes about thirty seconds to fasten and adjust. For someone doing multiple transfers a day, that matters. My mother goes from bed to bathroom to chair to table. Each time, the belt goes on. It has become just part of the routine.
If your parent can still push up with their legs at all, a gait belt is where you start -- not a transfer board.
The LiftAid belt has a metal buckle, multiple back loops, and runs sixty inches to fit larger patients too. It is the belt I use every day for my mother, and it is what most OTs recommend first.
Amazon Check Today's Price on Amazon →
Where the Transfer Board Wins
The transfer board wins when your patient truly cannot bear weight on their legs at all. This might be a patient with a complete spinal cord injury, a patient in late-stage neurological decline, or someone who has just had a lower-extremity surgery where weight-bearing is medically prohibited. In those cases, there is no leg drive to harness. The patient cannot push up. Asking them to is either futile or harmful. The transfer board fills that gap.
What a transfer board does is bridge two surfaces at roughly the same height -- wheelchair to bed, bed to toilet, car seat to wheelchair -- so that the patient can be slid across without being lifted entirely. When you have a truly non-weight-bearing patient and you need to move them laterally, a board is often safer than a pivot transfer because it removes the moment where you are holding all of their weight in mid-air. Boards range from basic smooth plastic to contoured versions with hand cutouts for the patient. The technique still requires training. The positioning, the angle, the way you protect the patient's skin from friction, the way you manage the board itself -- all of this takes practice. An occupational therapist should walk you through it the first time, not YouTube.
The weight-bearing line is the most important thing your physical therapist will tell you. If your parent has any weight-bearing capacity left, a gait belt is the right tool. The transfer board comes later, if it ever comes at all.
The Weight-Bearing Line That Decides Everything
In physical and occupational therapy, weight-bearing status has specific clinical categories. Full weight-bearing means the patient can put their full body weight through the limb. Partial weight-bearing means they can bear some percentage, often defined by the doctor -- 50 percent, for example. Toe-touch weight-bearing means the foot can touch the floor for balance but not for support. Non-weight-bearing means the limb takes no load at all. Most home caregivers are working with patients who are somewhere in the middle of that spectrum, not at the non-weight-bearing extreme.
If your parent is partial weight-bearing or better, a gait belt is the appropriate tool for standing transfers. The belt lets them use their own leg strength with your guidance. Bypassing that with a transfer board -- treating a partial weight-bearing patient as if they were non-weight-bearing -- can actually accelerate deconditioning. Muscles that do not work get weaker. Your occupational therapist will be specific about this. They will tell you what your patient's current weight-bearing status is and what tools correspond to that status. If you do not know your parent's weight-bearing status right now, that is the first question to ask at the next therapy appointment.
When an OT Graduates a Patient From Gait Belt to Transfer Board
The answer to 'which tool should I use?' often changes over time. A patient who starts as partial weight-bearing and does their home exercises may improve and no longer need the belt for every transfer -- they may be able to stand with just a grab bar. Or, if the condition is progressive, they may lose weight-bearing capacity over months or years and graduate to a transfer board. The occupational therapist makes that call, not the caregiver alone.
What I have seen in my own situation is that the OT re-evaluates at each visit and adjusts the plan. My mother went from needing the belt every time to now using it only for longer transfers and difficult surfaces. She no longer needs it to get off the couch if the couch height is right and a grab bar is nearby. That is progress. If she were declining instead of holding steady, the OT would be talking about a transfer board or a mechanical lift. The point is that these are not permanent decisions. They are current decisions based on current function.
One thing worth noting: many OTs will recommend you have both tools in the house if your patient is in a transitional period. They are not expensive, and having a transfer board available when you need it at 11 at night is far better than not having one. The gait belt will still be your primary tool. But the board is a reasonable backup if your patient has a bad day and cannot bear as much weight as usual.

Your Own Back: Why This Choice Matters as Much for You as for Them
Caregiver back injuries are one of the primary reasons family caregiving situations break down. The caregiver cannot continue, or they are injured badly enough to need care themselves. It is not talked about honestly enough. When you are pulling someone up from a low chair by their arm, or bending over a bed trying to reposition dead weight, you are loading your lumbar spine in exactly the way it is not designed to handle. Most of us find this out the hard way.
A gait belt protects your back because it repositions where you make contact with the patient. Instead of reaching out and up to grab an arm, you are gripping a belt that sits at the patient's center of mass. Your feet can be in a more stable position. Your core can be engaged. You can drive from your legs rather than torque from your spine. It is not a complete solution to caregiver ergonomics -- you still need to practice proper technique -- but it is a meaningful mechanical improvement over grabbing clothing or skin.
The transfer board protects your back differently: it removes the full vertical lift for non-weight-bearing patients and replaces it with a lateral slide. That can be genuinely easier on the caregiver, but the slide itself can still cause lower back strain if your technique is poor. The gait belt gives you a bigger margin for error on technique than a transfer board does. For caregivers who are new to this or working alone, the belt is more forgiving.
Who Should Buy Which
Buy the gait belt first if your patient can stand with assistance, can bear at least partial weight on their legs, or is recovering from surgery and is in the partial weight-bearing phase. This describes the majority of home caregiving situations. The LiftAid belt is what I have been using for two years. The metal buckle has not failed. The loops give me multiple grip options. At the current price, there is no reason to delay this purchase if you are doing daily transfers.
Buy or borrow a transfer board if your patient is medically non-weight-bearing, if your occupational therapist has specifically recommended one, or if you are supplementing a gait belt for days when your patient's function drops. Do not buy a transfer board to replace the gait belt for a patient who still has leg strength. You will be working harder than you need to, and you will be leaving your patient's leg muscles with less to do.
One tool that works on day one, costs under ten dollars, and protects your back every single transfer.
The LiftAid gait belt is 60 inches, has a metal buckle that has not given out in two years of daily use, and the back loops make it versatile for different patient heights and chair types. If you are doing standing transfers, this is the place to start.
Amazon Check Today's Price on Amazon →